I was introduced to this research method by Jamie Murdoch, Research Fellow, at the University of East Anglia (UEA).
The term sounds rather intimidating so let me say more about it as it will help some readers interested in research and ‘safe experimenting’
What is Linguistic Ethnography?
The term ‘linguistic ethnography’ is an umbrella term for specific approaches to research. Scholars combine linguistic and ethnographic research traditions to our understanding of the impact of our social world on us. It does not take for granted our ways of communicating on our everyday world (our ‘social context’, as it is labelled). Take a look at:
There is a connection here with the information I have provided about Acceptance and Commitment Therapy (ACT). I’m no great philosopher, but ACT authors have described their approach as based on the philosophy of science called functional contextualism. Put simply, this means focusing on things that work and the context in which they are working. You are likely to be less effective – and invite more small defeats – unless you design your safe experiments paying close attention to the context in which you are living your life.
As I see it, the research into therapy undertaken by Charles Truax and Robert Carkhuff, as well as later work on Neuro-linguistic programming, undertaken by Richard Bandler and John Grinder, emerged to some degree from this way of examining what goes on in our world.
…. and to safe experimenting
The relevance of linguistic ethnography to ‘safe experiments’ is that this research method serves to help us notice the social context within which we operate – just enough to see what changes might be made and how we might go about designing a suitable experiment.
You cannot do a safe experiment unless you want to do something different and, to notice what might be done differently, we need to notice the everyday impact on us of the world in which we are existing.
So, in practice, pay attention to the language you and others use and notice what impact language has on your understanding. Just as important, return to the Road Map safe experiment in How to Give Yourself a Nudge and notice how change is made difficult by our wider world.
The unintended consequences involved in ‘learning’ and adapting
Notice how others around us make it more or less easy to create change or even ‘allow’ us to become aware that change is feasible. Schools and colleges are intended to educate us; have you noticed how, sometimes, those institutions contain and reduce or ability to be different. It is precisely those ‘social contexts’ that may need disrupting before you can initiate a safe experiment effectively.
Do you remember the experiment about messages from our parents and grandparents? Most messages sent to us were meant to be well-meaning (sadly, not all). Go back to your records and notice the unintended consequences arising from some of the messages we received.
what was the impact on you? How did you respond to the outcomes?
In 2017/18, a group of clinical psychologists started a debate about the increasingly frail system of mental health assessment – processes used to label emotional and psychological ‘problems’.
The rather lengthy commentary, entitled Power, Threat and Meaning, can be found via:
I mention their work as they question the tendency to label behaviour and to see our responses as ‘problems’ in the first place. I want to offer a similar challenge here on my website; as an opportunity to review your life within the boundaries of your own …..
SPACE AND TIME, BODY and SPIRIT
I want my own approach to focus on the safe experiments only you can design.
I would go as far as saying that the Framework improves on my own perspective by making the POWER issue even more explicit. The Framework highlights the social setting in which we seem obliged to operate.
The Framework reminds us that we have to fit in to the world of other people, even if we only fight against the pressure to do so.
Sometimes we are oppressed by other people and sometimes we do the oppressing. It helps to be clear about this less comfortable aspect of the world in which we live.
Whenever you review your Road Map and Genogram experiments, please keep in mind where you fit in to your community and how you are treated in that wider world. I say, keep in ‘mind’, as your community is part of your mind!!
Limits of any Framework
Any Framework presents its own problems. It is still an attempt to explain what we do and where we fit in. This website seeks to reverse that process by asking: do you want to change and, if so, in what direction and, if so, how?
Rather than assume ‘a one size fits all’, my own approach assumes that you may fit in with the majority, or you may be in the minority or indeed, be a minority of one.
Other Frameworks and models seek to paint a picture of ‘Everyman’. I discuss some of them under Models informing Therapy. Such Frameworks are destined to fail (and not simply because ‘Everyman’ is now a sexist word!).
That said, some people I know rather like a label as it can provides a starting point. It can become a focus for initiating change. However, in my experience, others have been known to use the label as an excuse for doing nothing, made easier when an ‘expert’ makes a pronouncement!
Some possible lines to follow
Can the Framework foster safe experiments and story-telling? Try this, for instance:
EXPERIMENT: take a bit of paper and identify something current in your life – preferably a minor obstacle – and consider:
‘What happened to you [as you faced the obstacle]?’ (This may show how has Power operated in or on your life, e.g by a parent, teacher, manager or friend.
‘How did it affect you?’ Assuming the obstacle was a kind of Threat, what uncertainty did the outcome create in your life?.
‘What sense did you make of it?’ Elsewhere, I have said that humans may well be defined as ‘meaning-making creatures‘. So what Meaning did you make out of the outcome you faced?
NB As a seemingly brief experiment, this may be more difficult to complete than is first obvious. Give yourself time, if needs be; put things down and come back to your results, if needs be.
When you review your notes and results, consider: ‘What did you do, or are you doing to survive [that obstacle]?’ This identifies the responses you are making to the Threat?
Using the SWOT analysis
It’s an experiment that fits in to other elements on this web site. For instance, this framework picks up part of the SWOT analysis (Strengths, Weaknesses, Opportunities and Threats):
‘What are your strengths?’ (What access to Power resources do you have?)
…and asks if these questions help you know….
….. how do you deal with Threats?
Can you turn threats into Opportunities?
The results may well fit into the matrix illustrated here, if it helps.
Implications for the Script we ‘write’ about our life
These questions, and your answers, may help you construct some aspect of the story of your life (often called your ‘narrative’). In this web site, this ‘story’ is connected to the Script you have written for yourself on an unconscious level.
You can continue the experiment by considering:
‘What is your broader life story?’ and what changes, if any, do you want to make to that story and the way it is unfolding?.
It may help to return to your Road Map described early on in Ecograms and other Maps. This may help you develop your story from the various cross-roads emerging from your own road map.
Note how the Framework fits rather well into the cognitive behavioural models of change and the Transactional Analytic (TA) model, in particular.
Some key questions to consider when designing a safe experiment
If you want to continue the experiment, return to the TA questions.
Remind yourself about a current issue in your life, and ask:
What do you want (that is different)?
How will you get what you want (make it different)?
What stops you getting what you want?
Who or what do you need, in addition, now, to get what you want?
Such questions, in my view, help us to move things forward, rather than simply label a condition. Too often health professionals spend time on what is known as ‘assessment’ in order to search out an appropriate label. It can do more than that: assessment collects ‘facts’ relevant to your life story so you can be initiate change – get treatment, if you like.
Assessment, in my view, is best regarded as helping YOU to tell your story. Change may not be possible until that story starts to be told.
The Framework – as adapted and summarised here – is well worth a more detailed examination. It questions assessment in its traditional form, and modern practice.
It may cast light on what you understand about your current circumstances.
Most importantly, it is an approach that invites you to start formulating your way forward, rather than waiting to be ‘told’!
Recently I was asked: why provide this information for free? Doesn’t your living depend on it?
As an evolving ape, I am beginning to realise that there is an alternative to short-term profiteering from other people’s hardship and distress.
To explain what I am getting at here prompts me to comment on my motivation for writing up this extensive website.
For a start, I am writing it for me; I am gathering my thoughts at the tail-end of my career.
That said, I am confident that my story will help me talk to a different kind of ‘client’ or, indeed, a non-client (as well as old clients). There are people out there who are able to change themselves with minimal professional guidance. I will be happy enough if just one person makes a safe change in the direction of their life without consultation with me or anyone else!
Furthermore, in practical terms, my approach may increase the flow of business to professional therapists. Some people reading this material will do some experimenting and come to the conclusion that some professional advice may help. That is a ‘good thing’ as the first step along the path of change. It recognises that something needs to change. The individual can become more confident about how, and where, to find the help that will move things on. In the jargon of my professional world, this is termed resource-building!
By becoming more aware of what we need to do, and the obstacles to getting things done, we can identify our own conclusions and act on them. The most successful clients I have ever worked with are those who meet me for the first time after they have already started to make changes. By the way, the other factor that sticks out is CURIOSITY; a willingness to enquire and listen to the results, rather than love or hate them. You know who you are!!
One obstacle to change arises when we are told what conclusions to draw, and how to behave, based on those conclusions. For example, our families and life partners do this to us with the very best of intentions; they may well want only good things for us. Even so, their behaviour can have the unintended consequence of stopping us in our tracks – prompting some of us to rebel against what we are told! My wife will tell you that I am one of them.
There is a lot of difference between information that directs us toward something, and similar comments that simply point out, or guide us. Once we had spiritual teachers directing our behaviour from the pulpit, or its equivalent. Today we are much more able to assess information and make judgments for ourselves. Humankind has not been around so very long, but we are still evolving from a reactive being into a thinking self and, thereafter, to an increasingly self-directing human being.
Sadly, I am aware that this comes at a cost as some people initiate large and unsafe ‘experiments’ that endanger themselves and others around them. For the present, we still need laws to contain those disorganised individuals.
When you find that my material is interfering with your move toward self-direction – drop it! I am sure you will find something that does not work, just as there will be things that DO work.
Please let me know so I can review content. When I do help, I want it to be sure that I am only supporting you to devise changes that you want to make.
I have been asked how the ‘safe experiment’ model fits into our understanding of how we change.
This is a good point as some of the theory around change explains why we have to persist with some experiments and learn from results that leave us discomforted – those small defeats, I mention.
Effective change appears to require some initial inspiration, growing Motivation and an effective strategy that transforms into the ‘do-able thing’.
The results of achieving one do-able thing after another makes for change. If it’s the preferred change – then you will do more of it.
If it is an unexpected or undesirable change, then you will find something a little bit different to experiment with instead.
For a practical example of a change process, specifically relating to the research of James Prochaska and Carlo DiClemente, take a look at:
This material is based on important research contained in their text:
Trans-theoretical Stages of Change model (1983), with more information here.
Those pages, alone, along with material from people I have met, provide considerable practical suggestions for any number of safe experiments. TRY IT!!
‘Negative cognitions’ are phrases we have in our head – internal dialogue, as it has been called. ‘Negative’ as we usually bad-mouth ourselves and/or other people. This is a large topic to explore, but you could look beyond this website to:
Interestingly, I came to this web site late on. It builds my confidence to see that the key ideas are being shared out there by many in the ‘business’.
….. and a final one just so you can see common practices being offered here and there.
Would you find it of interest to explore the ways in which you can use these common ways of thinking to design the way that works for you.
There is a growing interest in ‘walking’ therapies that might be of interest:
HEALTH WARNING 1: beware of doing any exercise just because it is ‘there’, or some-one thinks its good for you.
Finding your own way is likely to be better matched to your life style, your foibles and abilities. The further advice I’d offer is for you to design any safe experiment in small chunks. Biting off more than I can chew tends to put my back out!
The reason why I came back to this page today, is that I have been asked about Guided Visualisation. There is material on this topic at:
and I’d mention the important health warning on this, and other web sites:
HEALTH WARNING 2: Use relaxation audio and videos wisely. Do not watch or listen to relaxation materials when you need to be fully awake and alert (for example, when driving).
Although it is obvious that this can be dangerous, cars are equipped with CD players and radios and none of us is exempt from drifting off under certain conditions.
Several people i know have found HeadSpace a useful internet resource. Take a look at:
This is a picture of the Greek, Socrates. He was an early therapist …. sorry, philosopher, who lives before Christ; before the Common Era (CE).
My web site places emphasis on action – getting something done. Socrates was not always too sure about action, any more than modern Buddhists are.
So here’s a bit of heresy against myself. Action is not always enough or appropriate to the moment!
How so, and when?
Doing is not always a respectable word in modern therapy. Action does not always ‘bring home the bacon’. Action can be a substitute for ‘real’ change in some situations – a handy disguise – a diversion. We can pretend to be changing.
Do you notice when you run around like the proverbial ‘headless chicken’, getting no-where very fast?
Ever heard of the French expression: “plus ça change, plus c’est la même chose“. Roughly: the more it changes, the more it’s the same thing.
Another block to effective experimenting
One reason why safe experiments may not work is that our cunning minds find actions-of-convenience that are, in truth, sneaky avoidances. One way to face this possibility is to use words, not actions. Socrates, an ancient Greek was great at this. Socrates was a philosopher and he had something useful to say about questioning ourselves and others. His famous sayings include:
An unexamined life is not worth living; and,
I cannot teach anybody anything, I can only make them think.
THINK, before Judging and Judge before Acting
So, you see, Socrates was keen on thinking before action! That’s why I suggest that the ancient Greeks had therapists on hand – oh, and probably sages from even more ancient civilisations.
As I understand it, Socrates was advising that actions assume we have made a judgement that so-and-so is a ‘good’ action. He is saying that such judgements assume we have thought enough to know what full range of options are open to us. In fact,
Socrates asserted that we cannot make a judgement about which option to follow until we’ve thought through the range of possibilities, and which ones seem most helpful.
As a by the way, this issue of how to identify our options is particularly important when life feels so rotten that there appear to be no options.
One safe experiment relating to thinking, instead of acting, is half-way down this page:
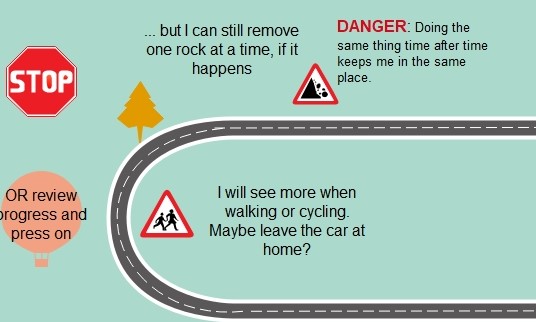
An alternative approach is to remember how many of us, as children, were taught the Green Cross Code – that is, how to cross roads. The aim was to stop us rushing out into the road using the mantra: STOP-LOOK-LISTEN. It is not easy simply to STOP, just like that, so anything that helps me to reflect – before I respond – can help. Elsewhere, I have touched on the value of CURIOSITY, as a quality that can make a difference in therapy.
Finally, the amended Chinese proverb on this page, relating to adult learning, may help us to see the greater value of ‘reflection’ in the scheme of things. Action is not seen as top of the hierarchy on that page!
Therefore, we can act, but that’s best done after we’ve judged the situation and that’s best done when we’ve exercised on our ability to think on things.
His great skill was theQuestioning Habit in his conversations with others (see item 7 for more practical ideas on ‘questions’ – way down the hyper-linked page). Socrates was argumentative and cross-examined others to improve our self-knowledge. He was said to be devoted to the truth so much so that he died rather than give up his philosophy and his home.
He was obliged to poison himself when a jury of his peers convicted him of being too clever by half! He believed in the power of reason and, after his conviction, he was said to have continued to argue about his fate after death.
He saw the sneakiness of his fellows and appeared to test himself to the death.
Watching out for our own sneakiness
To become more aware of our own sneakiness requires us to pay attention to our thoughts, beliefs, values and attitudes. In these areas, the experiments you may have to do are thought-experiments. Albert Einstein was the celebrity thought-experimenter and you can find out more about them at:
To work on inoculating yourself, try saying ‘hello‘ to your own sneakiness and just notice the ways in which you are sneaky. Notice all the benefits of sneakiness to you and consider whether sneaky may, indeed, help you from time to time and, if so, how.
When you find a way in which sneaky is getting in the way of your preferred change, go back to this web site and design a safe experiment once more. Let Socrates keep whispering in your ear.
One of the principles I have mentioned is that no ‘safe experiment’ will always work for everybody or even work always for some people. The most sensible thing to expect is that all experiments can work for some people, some of the time.
Sometimes it helps to think about things and to just notice our thoughts. A problem, when designing your own safe experiments, may well be to decide what to record and how to record it. So, now back to actions, once more.
As my web site has been around for some time, the number of pages has increased. As I have gathered feedback from readers and experimenters, I notice a regular question that arises is: is there evidence for the effectiveness of ‘safe experiments’?
I’m going to say ‘yes’ and ‘no’, aren’t I!?
The ‘yes’ is that all the information recorded by readers and clients over many decades constitutes ‘evidence’, in my book. Some of this ‘evidence’ is included on this website.
It’s a ‘no’ because the material is inconsistent – not replicable, by all and every-one. Yet, replication is a key feature of reliable and valid evidence. This troubles me less as my focus on is how you use the ‘evidence’ available to you. If you are troubled and struggling to learn from small defeats when the ‘evidence’ is difficult to follow, then your confidence may be undermined by that inconsistency. That makes it difficult to press on further down that scenic route.
It is but one ‘rock’ on the road. It can be overcome
Cognitive behavioural therapy (CBT) is a key model for encouraging experiments (or homework, as some call it). It encourages substantial record keeping, maybe too much for some people’s liking. Even so, such records do provide detailed information about the outcomes of all our efforts. Further, there is a large body of formal research seeking to organise evidence in books and PhD theses.
I am not an expert in research literature although I can see it increases at an alarming rate. Keeping it at my finger tips as one of my professional strengths. What I’d like to do on this page is to go back to that word – ‘evidence’. What is meant by it and in what way does it help us to design experiments and promote the changes we want in our lives?
There are some misunderstandings to identify and I’d like to clarify what is useful ‘evidence’ when exploring human experience and relationships (as compared to evidence obtained in laboratories).
The respect given to medicine in the ‘healing’ processes has meant there is pressure to define ‘evidence’ the same in both medicine and therapy. This is a ‘political’ pressure to join the ‘big boys’, given the dominance of medical science in the field of research.
Nathan Beel put it well in a 2011 Paper entitled What can we learn from what works across therapies? He stated that:
“The medical model and evidence based treatment philosophy is seductive in its appeal when applied to psychological therapies. They offer hope that a correct diagnosis leads to a treatment that will result in a cure or, at the very least, remission“.
He concludes that the over-emphasis on identifying a ‘superior’ model draws attention away from common factors between the many models that can lead to therapeutic change.
Don’t get me wrong; medical bodies and regulators are quite right to place emphasis on obtaining very solid evidence before they let a new medicine loose on the general public. There, the outcomes are matters of life-or-death, as I’ve said elsewhere. Often, only the strictest experimental design is put together. That seems quite right and there is little room for a Plan B or an opportunity to step back and re-design.
The Thalidomide scandal of the 1950’s and 60’s served to highlight the problems and to drive up standards in research.
There have been moves to improve the independence of staff involved in research studies as well. Despite all this, it is possible to manage, manoevre or plain manipulate research findings. The history of research financed by parties with conflicts of interest, e.g. the pharmaceutical industry, is littered with examples of this.
… and when it is not life-or-death?
However, this life-and-death feature is not present in the design and implementation of small, safe experiments, as I am describing them. The problem for measuring the effectiveness of therapy, using the tight controls associated with medical science, means that:
* useful data and results are sometimes excluded from research studies. For example, the experiments I am offering, and you will design, may have no visible result on some occasion. You can neither confirm nor deny your progress toward the objective under scrutiny at that time. Problem is, the same plan may well produce a different result on another day. What is ‘bad’ one time, may be ‘good’ or, at least, better another time.
* methods applied to the test of a drug are very different from tests we should apply in therapy. You can objectify a drug and make it a ‘subject’ of study. You can control that subject as tightly as you want. Good therapists do not objectify their clients. Effective researchers into therapy are ill-advised to try to do so. Indeed, the client is the primary experimenters, and the therapist more a guide. The good therapist will negotiate a preferred outcome – one a client wants – and one a therapist is equipped to help on its way. Then the therapist can help a client find a way towards that outcome. Research has to be able to focus light on how that process is initiated and sustained.
Evidence-based researchers say they follow ethical guidelines and that is all well and proper. Those guidelines exist to see ‘subjects’ are not abused. Even so, the key focus of medical research will be: did what we do to our subjects – in applying a treatment in ethical fashion – make people better? In therapy, it is not enough to simply assist people to get better; the way therapists help people get better so clients can continue that work once therapy is terminated. Achieving this outcome is central to the research in human relations. Ethics are more than a guideline to minimise the potential for abuse. How we behave towards one another is not an optional extra and yet what we do to move things on may involve some measured and informed risk-taking.
Ethical research into therapy should assess what works to ensure clients are respected. Furthermore, research can identify what negotiating and communications styles engage clients. The way a tablet is given to a patient does not usually impact on outcomes (but, again, there may well be evidence to contradict this assertion and I understand the ‘gold standard’ Random Controlled Trial (RCT’s) do, indeed, just that!
Research into therapy can study the validity and reliability of experiments but are the criteria to define these terms identical in the scientific and therapeutic environment. Now that is a BIG question. My short answer is, no, they are not.
The recording systems used by client and therapist could be assessed. Some may be more efficient than others in illuminating outcomes. But even then, effective therapeutic research identifies how the parties got where they did. It follows the journey from the design of a safe experiment through to observing its outcome and then interpreting and assessing the same. Research in medicine and science may ill-afford to study the journey; some people may die en-route and that is not acceptable.
so the ‘danger’ to clients in therapy is of a different order to the risks involved in medicine. Some people do challenge this, say, in relation to reports of ‘false memory’ syndrome, but problems of that order say more about therapists pursuing their own ideas, rather than enabling ‘clients’ to make the move that is right for them. That is not ethical therapy.
Once we can recognise that ‘safe experimenting’ is not what some-one else does to you, then it becomes much easier to look for ‘evidence’ that fosters incremental and fluid outcomes you obtain.
Furthermore, taking small steps in the implementation of ‘safe experiments’ assumes that we can step back from the result and decide to set off in a different direction. It is reasonable to consider that successful journeys depend on mistakes – or at least, noticing them. I would argue that our small defeats often teach us more than our small victories. Some folk say that there is no learning without mistakes: the bigger mistakes made, the bigger the lessons learned although there is a limit to that. For instance, see what Edmund Burke had to say in that topic (you’ll need to scroll down a bit!). Defining evidence relevant to small, safe experiments means it is necessary to legitimise the ‘moving of the goal-posts’. That is a ‘no-no’ in strict research work.
even when an experiment is a ‘small defeat’, things can be learned from the outcomes. As seen above, the strict assessment of evidence puts a negative value on ‘failure’ – some people even turns their noses up at Placebo effects. That cuts off a very large chunk of helpful research into ‘what works for whom’.
Strict research looks askance at my assurance: if it works, don’t knock it. Therapeutic research needs systems to define what is meant by ‘what works‘ as well as ‘what works for whom‘.
Research into therapy will find that what works with one person, and at one time, will not necessarily work for some-one else or a different time. Further, as I have said, we learn much from apparent ‘failure’. If it helps, take a look at my page on what might be involved in planning an end to therapy; doing that effectively requires gathering some evidence – but what sort, eh?
I have a suspicion that some researchers like to follow strict rules of research to affirm the neat and tidy outcomes needed to generate confidence in a new pill or procedure they have designed!!
The world of therapy is rarely that tidy and it will miss important things if it tries to be tidy.If you want to apply your thinking to this subject, how about seeking out your own definition of evidence-based research. The one offered by one website is:
Evidence-based medicine is the conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. [my bold]
Do you wonder if the client view is really integrated in the sentiment that “external clinical evidence” is seen as part of ‘clinical expertise’? Sound research too often appears to be drawn up by a conference of experts. Too rarely is a client understood to be expert in themselves and that value needs to be at the ethical core of any research into the impact of therapy and how it works.
All this asks: what IS “best”? Notice how the practitioner may get included in defining ‘best’, but note that it is his/her “expertise“, that seems central. This is not new thinking; consider Tom Douglas’ comment in relation to Groupwork Practice (in a 1976 text by that name). Douglas was concerned that lack of information and understanding might mean group members would be troubled by having “little or no help or guidance, and many unnecessary mistakes and many avoidable hurts will be committed” (p.4). This is the view of practitioner-as-expert. This is very different from my own view; we can, indeed, get hurt, and yet still learn from the experience. We can make mistakes and mistakes, of a certain order, can be valuable life lessons. Note, if you would, the word ‘unnecessary’ used in relation to mistakes. Who’s saying what is necessary or unnecessary? Does emphasis on ‘small and safe'” let the individual determine ‘necessary’ with minimal risk. Can we not live with the consequences when we experience small defeats?
I use this example, as the groupwork I recall from the 60’s and 70’s placed large responsibilities on the individual to speak for themselves. Yet, in the few words from Tom Douglas I can be sense the subtle removal of power from ‘clients’.
If you wish to investigate this question further then colleagues from my old haunts in the north-east have something to offer. Their report contains an interesting chapter on what clients have to say about therapy.
Do their findings match your own experience of being engaged with counselling and therapy?
For a more thorough review of ‘measuring’ the results of our work, have a look at Scott Miller’s blog on: