
Recently I hear Dr Lane Pederson talking about this approach to therapy. It is an approach that has become more adaptable over the years since Marsha Linehan developed the standard approach to DBT.
The header illustration shows the model seeks to incorporate a number of perspectives – from cognitive behavioural therapy (CBT), Rogerian practice, Mindfulness etc – the usual suspects, if the truth be told!
Lane Pederson’s perspective
He highlighted that there is ‘nothing new under the sun‘. I wish more educators and trainers would accept this observable truth when teaching about therapy. He made the refreshing comment that he might be an ‘expert’ in DBT, as a therapy, but his therapeutic contribution is only good when a client or trainee discovers their own perspective. Success, he said, was putting DBT through your own ‘filter’.
That is true of all the small, safe experiments described throughout this website.
That said, he identified DBT as a highly structured approach to therapy. In his programme, he described the rules and expectations, and the safety skills, on offer in the model as well as the ‘hierarchy’ it uses. This ‘structure’ went on to present problems for me, as I will identify latger on. In the meanwhile, I will leave you to research that dimension of DBT, if you wish. I want to focus on the do-able things that you can use in safe experiments.
What was particularly refreshing was his en passant statement that therapists are better off adapting their own model of change to the one presented by the client. Here he was aware of the uniqueness in each relationship. Given his pre-occupation with labels and diagnoses elsewhere in the talk, I can only assume this is part of his dialectic: let’s have labels on the one hand and individualised and negotiated treatment on the other hand!
Also, he was ‘strict’ about boundaries holding little truck, for example, with time boundaries (lateness for therapy sessions). He seemed to have little interest in our ability to ‘just notice’. His advice was to stop “backsliding” and show “commitment” instead.
Now who is saying what at this point? True, he was talking about ‘abstinence’, and he asserted that abstinence was the goal of therapy. He did accept that small steps would help reach that goal and each client might have a different view on the timescale and skills that might help.
Also, he was’strict’ about his client’s time boundary management. My own view is ‘five/ten minutes either side is fine with me‘; and very few visitors breach that. Few are willing to lose that five or ten minutes, so the testing-out opportunity is rarely tested out! Even so, my attitude does enable some people to use time boundary management as a safe experiment. Lane’s does not.
Lane justifies his stance as not practising ineffective strategies in a session. Who judges ‘ineffective’ here? Do no mistakes have something to offer? Are all mistakes ‘ineffective’? Meeting clients may not help when a lot of rules are pre-set or taken as a given.
Tension and contradiction is OK!
Sounds contradictory, does it not? Do your own thing within this hierarchy!? That is the challenging thing about DBT! It thrives on contradiction! The language of DBT fosters the crossed transaction that is created by contradictions in human conversation. It emphasises choice (between seeming opposites) and arguing about them to create even more choices.
The DBT ‘attitude’ is that no position is absolute even if Lane’s rules sounded rather like that. Each person formulates their world with their own kernel of truth. Lane was less keen on ‘yes, but’, and more attentive to ‘yes, and…’. He wanted therapy to integrate opposites, and find ‘what’s missing’ in order to find a workable balance.
He saw Dialectical behaviour therapy (DBT) as an evidence-based psychotherapy that began with efforts to treat personality disorders and conflict. DBT focuses on a process in which the therapist and client negotiate different change-oriented strategies. Through this, they can interact and integrate opposites by balancing them out (hence the label ‘dialectical‘ – reaching a synthesis through argument).
DBT was designed to help people increase their emotional and cognitive regulation by identifying and managing unwanted triggers through the development of different coping skills. That’s something I share when it comes to establishing a purpose for therapy – so the quarrel may be with the ‘how’ of to acheive it.
My own perspective
….. encourages you to argue with yourself, and a therapist if that helps. Use the argument to just notice the evidence emerging from a number of your own small, safe and specific experiments. I do not see it emerging from some-one else’s structure used in an unquestioning fashion.
How come? Look at this illustration to see what happens when we hand over our power to others.
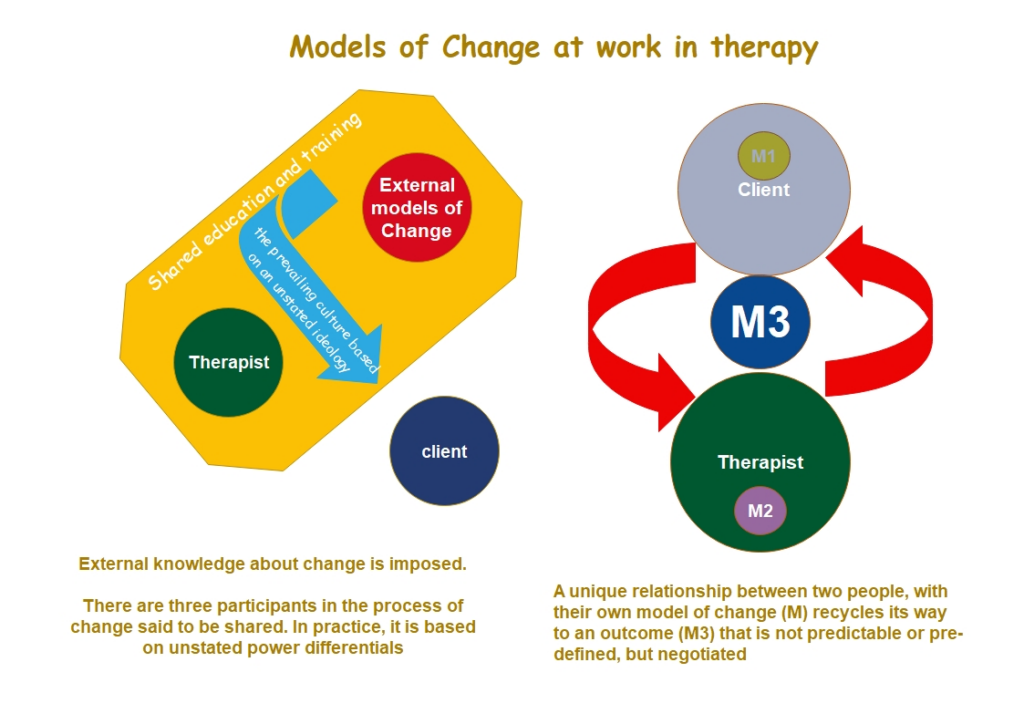
The illustration says you can accept the boundaries set by others. Alternatively, you can choose what works for you, from all that is available. Work with another person to create the tension and test out and negotiate new and unique approaches to change.
Neuroscience
DBT shares with Dan Siegel, Peter Levine, Babette Rothschild, Pat Ogden and van der Kolk, and others, an interest in the neuroscience of emotions. The way our emotions play out can create one of the vulnerabilities that arise from the human experience. Some of these vulnerabilities arise as our Minds emerge from a complex set of reciprocal relationships between our brain, body, our environment, and the people in it.
I’m OK with this perspective as long as those ‘vulnerabilities’ do not place the client in a one-down relationship when in therapy as represented in my illustration, above. After all, when I am in a therapist-role, I still possess ‘vulnerabilities’. Too often, in my experience, this is denied and that is not good in a therapist.
Let’s relate this to some safe experiments
Here are some website leads to start you off:
What happens to our Autonomic Nervous system (ANS) when we use controlled breathing.
Emotional Regulation: Lane sees DBT as paying attention to self-care and regulation from the very start. He sees this as skills training in order to gain mastery. Personally, I see it as giving insight into controls we possess, and think we may not have. Controlled breathing is a ‘gateway’ to so many others things, such as active relaxation, meditation, exercise and the art of slowing down. The following pages also have things to say about suitable safe experiments:
Acceptance: see Acceptance and Commitment Therapy (ACT)
Compassion for self and others: Compassion Focused Therapy (CFT)
Approaches to change: see Models of Change
Communication styles: see Communication: it’s not what you say, but the way that you do it
Let me offer some specific safe experiments for your consideration.
Actions and movement: see Safe experiments when the talking has to stop and Expressive Arts can start. Increasingly, this website offers encouragement to act, not rely on talk.
Further reservations about Lane’s view
Lane sounded not at all keen on relapse. He appeared to deny relapse might prove a useful part of therapy. On one occasion, he said: we need to go all the way …. give things up 100%. Lane gave the example of a client saying “so relapse is part of recovery” and he denied this with several emphatic no’s. It was as though small defeats were not permitted, leave alone available to learn from! Here I disagree with Lane. For me – relapsing can be a learning opportunity – just one of many obstacles. Our ability to manage small defeats may help as least as much as victories.
Lane has a background in therapeutic approaches to personality disorders. I was unsettled by this. It’s my experience that cognitive perspectives seem to have a natural attraction to labels. Maybe this serves to simplify our understanding of what is in front of us and focus on what is changeable.
Would that it worked like that. I do comment on ‘labels’ as helpful to some clients, but I have reservations about therapists using them too freely. Too often that pre-occupation diverts the therapist in a certain direction – of their own choosing. This seems especially true with the use of ‘lazy’ labels such as Borderline Personality Disorder and Obsessive Compulsive Disorders or Attention Deficit etc. I say ‘lazy’ as these labels can deter both parties from considering what is actually happening to a given individual.
At one point he identified differences between therapies saying “CBT is thought-focused whereas DBT is emotion-focused“. What he may have intended to say is that DBT is, on the one hand, thought-focused and emotion-focused on the other hand! Effective communication rather depends on both foci being integrated one with the other.
Also, Lane’s input focused a lot on Mindfulness and highlighted some myths about this approach to self care.
After I started on this page, I found this poem in a totally different place. What do you think of it – as a light shone on the DBT perspective:
The boat will sway
Jaswant Singh Neki, with an extract from a Punjabi metaphysical
The impatience of people yearning for shore, one way,
The will of the restless waves pointing the other way
To which side the boat will glide?
Whichever shore, wave ‘consents’ to meet
Whichever shore the ‘unchecked’ winds greet
Is the way, the boat will sway
poem, translated from the Punjabi by Dr. Raman Deep.
My source is: Di Nicola V. The Gur??Chel? Revisited: The Contemporary Relevance
of the Work of Indian Psychiatrist Jaswant Singh Neki in World Soc Psychiatry 2022; 4:182-6.