
I have been told that my approach is person, or client-centred. To some extent this has to be true in the sense that any effective therapist has to demonstrate respect and positive regard for the person in front of them.
That said, I am not convinced that I am ‘person-centred’ in the traditional understanding of the ‘person-centred school’. This perspective can be tracked back to the work of Carl Rogers (assuming you do not want to travel back to the Greeks!).
Carl Ransom Rogers (Jan 8th 1902 – Feb 4th 1987)
You can find a summary account of Rogers’ life and work at:
https://en.wikipedia.org/wiki/Carl_Rogers
…. with more background on offer at: https://counsellingtutor.com/
Some reservations
The reason why I am reluctant to accept a person-centred label is that I may adopt an humanistic stance in my work, but that’s a rather broad term that casts little light. Even then, I even raise doubts about the humanistic work of Maslow and others.
In my actual professional practice, I place large demands on my ‘clients’ that may encourage client-centred colleagues to look askance at my approach.
Rogers’ Conditions
Rogers’ core conditions (not his term, by the way) began to emerge in:
Rogers, C (1957) The necessary and sufficient conditions of therapeutic personality change in the Journal of Consulting Psychology
….. although his 1977 text, On Becoming a Person is more accessible.
How many ‘core conditions?
It is my view that his clear and incisive writing have become misunderstood and misinterpreted over many years. When I say this, I am referring not only to his three core conditions that are well-known, but also to three of less well publicised conditions:
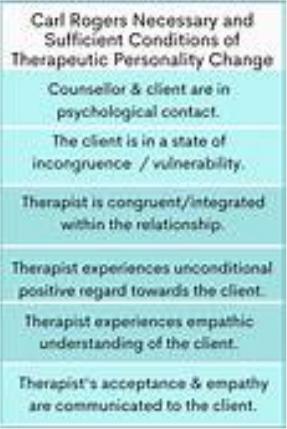
A summary of the six ‘conditions’
My understanding of this summary illustration of the six conditions, in brief, is:
1. that a relationship between client and therapist must exist and that each person’s perception of the other is important.
2. that incongruence exists between the client’s experience and awareness. This is a normal human condition, but one that motivates clients to seek to change. Does the therapist’s incongruence add to this ‘motivation’ to change?
3. the therapist needs to be congruent within the therapeutic relationship. That means the therapist is not “acting”. They can draw on their own experiences to facilitate the relationship. Traditional therapies were doubtful about therapists’ sharing their own experiences so Rogers was breaking ground here in the mid-20th century.
4. the therapist accepts the client unconditionally, that is, without judgment, disapproval or approval. This facilitates increased self-regard in the client, as they can begin to become aware of experiences in which their view of self-worth was distorted by others.
5. the therapist seeks to experience an empathic understanding of the client’s inner world (or internal frame of reference, as it is termed). The plan is that a therapist’s accurate empathy will help the client see the therapist’s unconditional regard for them.
6. The client perceives, at least to a minimal degree, that their therapist demonstrates unconditional positive regard and empathic understanding is present. Here is a neglected condition; I wonder why that is?!
Therapists are not good at asking if they do demonstrate those qualities and skills. I can be like that as the Be Strong Driver played a large part on my life.
Problems arising from interpretations of Rogers
My view is that translations of the six core conditions used by trainers has still minimise the relevance of testing a therapist’s knowledge and world-view.
In my opinion, the ‘problem’ that has emerged over the years stem from the neglect of that very first ‘condition’; being in “psychological contact“. This quality is discussed in some detail by this website. It’s worth just noticing what Rogers says in in 1957 Paper:
‘The first condition specifies that a minimal relationship, a psychological contact, must exist. I am hypothesizing that significant positive personality change does not occur except in a relationship. This is of course an hypothesis, and it may be disproved.” [my emphasis]
(Rogers 1957)
Negotiating a viable level of ‘psychological contact’
For me, psychological contact means that individuals are willing to enter a relationship possessing many dimensions. Just one dimension is a negotiated and viable level of psychological contact.
Equally important, that first condition assumes there is further sharing of our understanding of:
- Our individual psychological states and our level of understanding or insight.
- Our mutual understanding of the psychological states being created in this unique and fluid relationship created once a therapy contract has been drawn up.
The relationship is ever-changing as well as “an hypothesis” (see Rogers’ quote). That’s why I make several statements about ‘relationships’.
What about this one?
Too often we live our lives through IDEAS about our relationships, rather than within that relationship.
https://your-nudge.com/supervision-consultation-and-accountability-in-the-world-of-therapy/
It is this provisional and fluid understanding that makes therapeutic work slippery – almost beyond rule-making. There is a unique quality in each and every working relationship. In this respect, Rogers’ anticipated the late 20th century pre-occupation with unique processes. I mention Luborsky, Levitt and Norcross – and several others – on a few pages.
What this website seeks to do is to simplify this process and enable each reader to develop their own thinking, feeling and being – through a series of opportunities to explore and find out what works for you.
Whether you then take that inner psychological ‘contact’ into therapy with another is left up to you.
A therapist needs to develop skills and use them
There are further complications relating to Rogers’ notion of ‘psychological contact’. In my experience, clients do expect their therapists to use their knowledge and skills – and be active in using them.
One such skill is the judicious use of psycho-education. In my experience, clients do not expect knowledge and understanding to be withheld from them in the name of ‘unconditionality’, simply because they have not asked for it. That said, it pays for a therapist to know and act on a ‘no‘ when they hear it.
That’s trickier than it looks. As the Johari Window and the Discount Matrix demonstrate – it is difficult for any of us to ask for what we want when we do not know what to ask for!!
Can you identify and translate in a knowing way?
If you and I are ‘not knowing’ what are translations are today, then we simply collude with the 21st century of interpreted versions of the six core conditions. There is little chance of ‘abolishing’ incongruence within the therapist and other. Such incongruence is asserted to be unhelpful and unwanted. I am used to colleagues saying these issues, as listed, are addressed by the condition of ‘congruence’ within the therapeutic relationship. Such statements give the impression that the therapist has permission to speak their mind, and discouraged to put on a professional veneer.
Would that this were so.
This website infers that there is a lot of learning in the small defeat that is ‘incongruence’; where-ever it is located! You could just as well say the emotional dimension to all human decision-making can be abolished as well; but no-one I know can tell me how to do that as yet!
This ambition to abolish or control inconsistency is in my own view, not only unreasonable, but it actively impairs the working relationship. This is achieved by propagating one of the biggest discounts that human frailty lives with – even within professional relationships!
George Lehner made a good point about this.
A genuine therapist will experience small defeats, as well as small victories
In the ‘safe experimental’ method, a therapist will experience small defeats and small victories, as will the client. Each and every one needs to be available and explored in therapy – between sessions, and in the process of clinical supervision. Such defeats cannot be available until they are identified.
Some people would argue that this feature is recognised in the world of therapy; that’s why the profession created compulsory supervision (at least, in the UK). What the profession is more coy about is the fact that the same frailties exist within the supervisory relationship. The feature I highlight simply echoes through our culture, education systems and intimate relationships.
The implications of that are too troubling for the profession to face
So why is this feature so important? It is not reasonable to expect clients to identify and use their own small defeats and small victories if I, as a therapist, am unwilling to do the same thing. It is not simply a question of setting a ‘good example’: it is demonstrating by example.
On one final point, I would make is that self-regard in a client is increased not simply by gaining insights into your own current self-worth. They will also be enabled to do this when your therapist identifies how their own self-worth is distorted by self and others.
The impact of training
What I have observed, in training and in practice, is that modern therapists have swapped the ‘professional face’ of traditional 20th century therapist for a reluctance to ask questions or to offer an opinion. A potential small, safe experiment provided by a therapist is often frowned on.
For example, there is a time for “acting as if” when being a therapist. If a client appears to say something important, I can be tempted to speak out. I can, however, mark it with a non-verbal response. The latter are often powerful but they still require a conscious response from me – to a degree that is ‘acting’. I am not responding from some notion of a ‘true self’. Some of what I am saying emerges from Neuro-Linguistic Programming (NLP) – a model demonstrating there is an OK side to ‘act as if’.
Ideas of relationships are not good enough
In my view, over the years, the person-centred tradition lost the provisional and hypothetical spirit of Rogers’ writings, as well as his set of ethics. Training and trainers became wedded to the ideas behind the core conditions but an idea of a condition is not the same as demonstrating a therapeutic fundamental.
In time, ‘person-centredness’ became a defined quality and, in doing so, it lost the flexibility that Rogers’ installed into his hypotheses. The model slid into a ‘school’ – a rather ossified institution – and one that rather assumed that ‘clients’ can benefit from the therapist’s ‘respect’ for the core conditions, often without a negotiated limit of time.
In my own view, I trust most ‘clients’ will say that they permitted me to join them in an shared, negotiated journey – for only as long as that works for them – and with the intention, from the start, that our work will finish.